Perceptions
Children and adults affected by Infantile Nystagmus Syndrome, as a large percentage of individuals with Blue Cone Monochromacy, typically perceive the world similarly to other people without nystagmus, albeit with some degree of blurriness. Conversely, individuals with nystagmus that develops in adulthood often describe a sensation of movement or “shaking” in their visual field, known as oscillopsia.
To Learn More
Causes of Infantile Nystagmus Syndrome (INS)
INS is caused by a failure of the ocular motor system, the part of the brain that controls eye movement, to keep the eyes stable during the pursuit of a slow target. See ref [1] Chapter 1 and Ref. [4] for an introduction to the ocular motor system.
There are four basic types of eye movements – ref [1] Chapter 1 -:
- saccades, that are ballistic, conjugate eye movements that in a fast way change the point of foveal fixation. These are the fastest eye movement, 250-800°/sec with 200milli sec of latency. For example, you use saccades to point a target, to make a rapid re-fixation of a stimulus. It allows you to identify a target in the visual field with voluntary ocular movement and bring it into the fovea, carrying out foveation;
- smooth pursuit movements, are much slower tracking movements of the eyes designed to keep a moving stimulus on the fovea. For example, you use smooth pursuit movements when you follow the horizontal or vertical movement of a slow target; 0-30° per sec with a latency of 125 milli sec;
- vergence movements, that is disjunctive movements of the eyes (convergence or divergence) that align the fovea of each eye with targets located at different distances from the observer. You use vergence when you fix on an approaching or receding target; and
- vestibulo-ocular movements, that stabilize the eyes relative to the external world, thus compensating for head or body movements. If you fix a target and turn the head you are using these movements. Optokinetic movement is similar, and tracks images of the world during sustained world or background motion.
The accurancy of movements 1) – 4) are not affected by INS and the efficacy and quality of the movement is almost the same of individuals with and without INS. During periods of foveation, individuals with INS can maintain fixation as precisely as people without nystagmus [3]. However, we note here that vergence movements are able to stop nystagmus.
Nystagmus is related to movements 2). Let’s consider the smooth pursuit system inside the eye motion system.
The pursuit system is a delicate system with a damped oscillation. Once the target has been inserted on the fovea – foveation – the eye fixes it – fixation – and if the target moves making movements with various low speeds and accelerations, the eye is able to follow the target keeping it on the fovea to see it in detail and chasing it, adapting to its speed. The developing ocular motor system (OMS) requires good visual input to calibrate properly, and INS arises from a failure to calibrate a subsystem that is already borders on instability (i.e., oscillatory behavior) in normal humans. This failure to calibrate can be triggered or be associated with inherited or acquired medical conditions.
Let’s see what is a damped oscillation.
If you have a mass attached to a spring, with respect to the equilibrium position at x=0, moving the mass by an amplitude A, in the absence of friction, it will begin an oscillation around the point x=0 with a period T.

We note that we can visualize this motion in the next figure, with the case b=0 (absence of viscous friction) as a harmonic motion, in which during time t the mass m continuously oscillates between +A and -A. The extreme points +A and -A correspond to a velocity of the mass equals to 0 and to a reversal of the motion. The point x=0 corresponds to the point of maximum speed. In our eye system, the point x=0 is the target, and the oscillation is the nystagmus. Nystagmus cannot be considered a compensatory symptom of a sensory deficit, because it produces a vision handicap, given that the the eye oscillates between 0 and maximum velocity while fixating a stationary target.

Red line: over damped system
Orange line: critical – this is the fastest route without oscillation
Blue Line: under damped system
In individuals without nystagmus the smooth pursuit system is calibrated to have a damping force such as viscous friction, capable of damping the oscillation and tracking the target as it moves.
There are several models of the smooth pursuit system that have been developed, see for example Ref.[4] . These models try to obtain the velocity of the eye as a function of the velocity of the target, and they try to reproduce the high performance of this system to pursuits a slow moving target and its short latency time between the stimulus movement and the eye response, that is the eye velocity.
Can Blue Cone Monochromacy or other retinal diseases be considered a cause of nystagmus?
No. Some genetic diseases of the retina, such as Blue Cone Monochromacy and Achromatopsia, lead to low vision from birth. Individuals affected by these pathologies may present involuntary eye movements during the first year of life which in some subjects persist into adulthood and can be classified as Infantile Nystagmus Syndrome (INS). According to Dell’Osso it is not possible to detect a cause and effect condition between visual impairment and INS, because for example, for the same retinal disease there are individuals who show nystagmus and individuals who do not have it.
For example, we report the pedigree of two families affected by Blue Cone Monochromatism, a disease transmitted on the X chromosome, for which an average of approximately 5 individuals per family are affected according to data from the International Patient Register www.BCMRegistry.org. From the pedigrees we note that a large fraction of individuals, approximately 45%, show INS.



Muscles and Cranial Nerves involved in Nystagmus
The coordination of eye movements, including fixation, involves a complex interplay of neural circuits within the brainstem and higher brain centers. These circuits integrate sensory input, visual information, and motor commands to ensure precise control of eye movements and maintain steady gaze on a specific object or point of interest. There are six pairs of eye muscles and three pairs of cranial nerves that control eye muscles involved on eyes movements.
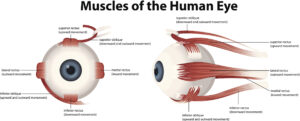
Eye Muscles
There are six muscles that enable the eye movement, the superior, inferior, medial and lateral rectus and the superior and inferior oblique:
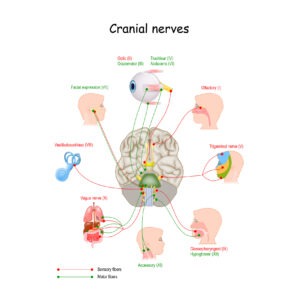
Cranial Nerves
There are 12 sets of Cranial Nerves (CN). Among them, there are three pairs of cranial nerves that control muscles of eye movement (each eye is controlled by one nerve of each pair). Damage to these nerves can interfere with eye muscles, and are associated with nystagmus. This is not the case of the nystagmus in Blue Cone Monochromacy and Achromatopsia, where usually there aren’t damages in Cranial Nerves. The rest of the nerves in the body emerge from the spinal cord but all the cranial nerves come from the brain.